


Purpose
Infant acute lymphoblastic leukemia (ALL) is characterized by KMT2A gene rearrangements and a poor outcome. Therefore, infants are treated with specific protocols. In older children, minimal residual disease (MRD) is used for risk group stratification. In infant ALL, data on MRD are scarce. We evaluated the prognostic value of MRD in a large series of infants with KMT2A rearranged ALL, treated within Interfant-06 in order to establish how to use MRD in these patients. This protocol included a randomization between lymphoid-style consolidation (protocol IB) versus a myeloid-style consolidation (ADE/MAE).
Patients and methods
MRD was measured in 249 infants with KMT2A-rearranged ALL by DNA-based PCR of rearranged KMT2A, immunoglobulin and/or T-cell receptor genes, at end of induction (EOI) (n=210), end of consolidation (EOC) (n=173) and after MARMA (n=164). MRD results were classified as negative, intermediate (<5x10-4), and high (≥5x10-4).
Results
In samples with both data on KMT2A MRD PCR and IG/TR MRD targets available (n=223), results were concordant in 94% (n=210/223) of samples.
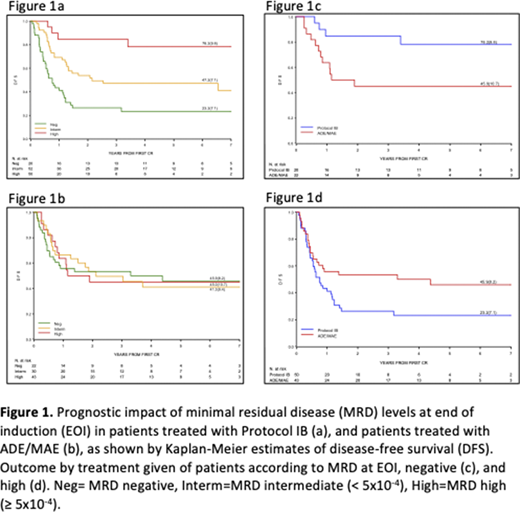
EOI MRD levels predicted outcome with 6-year disease free survival (DFS [SE]) of 60.2% (7.9), 45.0% (5.6), 33.8 % (5.3), for infants with negative, intermediate and high EOI MRD levels, respectively (p=0.0039). Strikingly, when analyzing MRD results according to consolidation treatment given, MRD levels at EOI predicted treatment outcome for patients treated with lymphoid-style consolidation, but not for patients treated with myeloid style consolidation. In patients treated with lymphoid-style consolidation 6-year DFS (SE) was 78.2% (9.8), 47.2% (7.1), 23.2% (7.1) for negative, intermediate and high MRD levels, (figure 1a) respectively (p<0.0001), whilst in myeloid-style treated patients the corresponding figures were 45.0% (10.7), 41.3% (9.4) and 45.9% (8.2) (figure 1b)
This implies that patients with low EOI MRD benefit from protocol IB lymphoid consolidation (DFS 78.2% versus 45.0%, figure 1c), while patients with high MRD benefit from ADE/MAE myeloid consolidation (DFS 45.9% versus 23.2%, figure 1d)). In line with these findings, co-expression of myeloid markers was found in a higher percentage of patients with high EOI MRD (81%) versus those with low EOI MRD (50%) (p=0.0186).
EOC MRD levels were also predictive of outcome, with 6-year DFS of 68.2 %(5.8), 40.1% (6.2), 11.9% (8.7) for infants with negative, intermediate and high EOC MRD levels respectively (p<0.0001). Patients that had positive EOI MRD and became negative at EOC also had a good outcome (6-DFS (SE) 65.7% (7.8))
Conclusion
Induction therapy selects infant ALL patients for the type of subsequent therapy; infants with high EOI MRD benefit from AML-like consolidation, whereas patients with low MRD benefit from ALL-like consolidation. This hypothesis is further supported by the more pronounced expression of myeloid markers in patients with high EOI MRD levels. Patients with positive EOC MRD had dismal outcomes. These findings will be used for treatment interventions in the next Interfant protocol.
Brethon:Amgen: Other: invitation to meetings, remunerations for oral presentations, advices for the record of Blinatumomab in pediatrics in France. Locatelli:Jazz Pharmaceeutical: Speakers Bureau; Medac: Speakers Bureau; Miltenyi: Speakers Bureau; Bellicum Pharmaceutical: Membership on an entity's Board of Directors or advisory committees; Novartis: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau; Amgen: Membership on an entity's Board of Directors or advisory committees, Speakers Bureau.
This icon denotes a clinically relevant abstract

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal